





Implants 101
Download PDF Version of these Instructions
Implant Terminology

Dental implants are precisely engineered, FDA-approved medical devices made from highly biocompatible titanium. The modern implant design has been refined by numerous iterations over the last 60 years. Dental implants consist of 3 basic components: the implant body (4), the abutment (3), and the crown (1). The implant body is the screw-like fixture placed by the surgeon into the jaw bone where it serves as the permanent foundation for a crown. Connecting the crown to the implant body is the abutment. The abutment connects to the implant by screwing (2) into the internal threading inside the implant body (and can therefore be un-screwed if needed and removed or replaced). Prior to placement of the final crown a type of abutment called a healing abutment may be placed on the implant body. The healing abutment helps to mold and sculpt the healing gum tissues in the area of the implant to prepare the site for it’s final crown.
Osseointegration
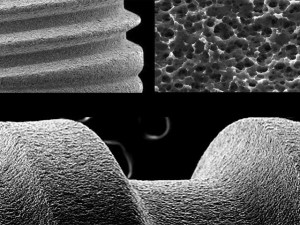
A successful implant is a stable implant. The implant must be rigidly fixed and not move when chewing and biting (just like all other teeth). An implant’s initial (“primary”) stability is achieved by the binding of the external threads of the implant body into the bone (just like a screw placed into wood). However the final stability (and therefore, the long term success) of an implant is due to osseointegration of the implant with the surrounding bone. Osseointegration is defined as the direct structural and functional connection between living bone and the surface of a load-bearing artificial implant. During osseointegration the bone surrounding an implant grows into the numerous microscopic irregularities designed into the implant surface. Just like countless small hooks in Velcro provide enormous holding power, numerous microscopic and intimate implant surface interactions with the surrounding bone provide great strength to a dental implant. Importantly, the osseointegration process is a physiologic process! It takes 3-6 months to complete. This is why implants “take so long;” we’re waiting on a physiologic process to complete and it just takes time.
The 4 Bone Types of the Jaw
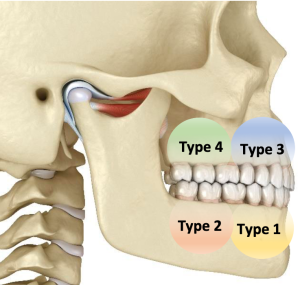
Every implant is unique based on its particular structural and functional requirements. No two cases are the same. However, treatment planning for implants is generally organized conceptually by the “type” of bone into which the implant is placed. There are 4 different “types” of bone in the mouth. These different types are based on bone density (i.e. the amount of calcification in a given volume of bone). Highly calcified bone is generally the most successful for implants because it tends to hold the implant tightly. Bone that is low in calcification (and therefore higher in marrow content) is less favorable for implants because it holds the implant less tightly than highly calcified bone would. Type 1 bone is the most calcified (“hardest”) and is found in the front of the lower jaw. Type 4 bone is the least calcified (“softest”) and is found in the back of the upper jaw. Types 2 and 3 bone (back lower jaw and front upper jaw, respectively) are of intermediate density. Each type of bone has different considerations for implant placement. (Sometimes it’s helpful to think of these different densities of bone like different types of wood: type 1 bone is very dense and hard like oak or walnut, whereas type 4 bone is very soft and pliable like pine or balsawood.)
Moreover, the upper molar tooth areas (Type 4 bone) are further complicated by the presence of the overlying maxillary sinus, which often requires bone grafting for implant success. For these and other reasons, each implant is different. So if you’ve had a different experience with a previous implant or if you know someone who had a different experience (even if it’s the same tooth that needs to be replaced!), you now know that there are many factors that make every implant unique.
Challenges to Success
Most people are candidates for implants. There are a few circumstances that adversely affect the probability of implant success. Circumstances that may jeopardize long-term implant success are typically due to factors that alter normal bone physiology. Things which are known to alter normal bone physiology in the jaw bones include poorly controlled diabetes (HbA1C > 7.0), history of radiation to the face/neck, ongoing or planned chemotherapy, genetic disorders of bone, long-term steroid use, medications used to treat autoimmune disorders, and medications used to treat osteoporosis. It should be stressed that each case is different, and your particular case deserves a careful, individualized consideration of all factors that may affect implant success.
Functional Requirements
Temporary crowns are used on implants to maximize the esthetic outcome. Therefore temporary crowns are used when implants are inserted to replace missing front teeth where esthetics are paramount. Back teeth (molars) primarily serve a functional purpose: they’re meant to do the “heavy lifting” of day-to-day chewing. Esthetics (while still important) is secondary to function for back teeth. Therefore temporary crowns are typically (although, not always) not used when implants are inserted to replace missing back teeth. Premolar teeth are located between the front teeth and the back teeth. Their role is intermediate; half esthetic and half functional. Sometimes premolar implants require temporary crowns, and sometimes they don’t. Again each case is different and requires careful attention to detail and individualized treatment planning.